
Suddenly Hearing Loss: It’s A Medical Emergency!
What should you do if you suddenly lost your hearing? See your ENT doctor as soon as possible! If the hearing loss is severe, it’s not going to be due to “just earwax”! Sudden hearing loss is a rare but serious ENT condition in Singapore. We see 3-4 cases every month at our busy ENTcare specialist clinic. Sudden hearing loss is an emergency so you need to seek treatment urgently. This should ideally be within the first 72 hours of your sudden hearing loss.
I remember writing a review on Sudden Hearing Loss in a peer-reviewed ENT academic journal (AC Leong et al, Clinical Otolaryngology, 2007, Pubmed ID 17883561). Let me summarise it for you.
WHAT ARE THE WARNING SIGNS OF SUDDEN HEARING LOSS?
Sudden hearing loss is a very distressing condition for the patient as it presents with a sudden severe blocked ear sensation. This is often associated with severe ringing or tinnitus in the affected ear. It may also cause vertigo and dizziness. Patients don’t feel any ear pain but may describe a sudden “vacuum” feeling in their ear. The initial dizziness often settles down but tinnitus and blocked ear symptoms may remain.
With only one good hearing ear, patients struggle to hear in noisy places. They have a lot of difficulty trying to localise sound . This means that they cannot tell where the sound of interest is coming from. It is challenging in social situations with many people talking at the same time. You won’t be able to hear the voice of the person you want to focus on. You may also unintentionally ignore the person speaking to you on the side of your bad ear, which can be socially awkward.
WHAT CAUSES SUDDEN HEARING LOSS?
Although many cases do not have a clear cause, some patients report having had their ear exposed to loud noise before losing their hearing. Others recall having had the flu or some viral infection of the nose before they lost their hearing. Sudden hearing loss mostly occurs in in just one ear but it can also affect both ears at the same time. In bilateral cases, patients tend to have other health conditions. For example, auto-immune conditions such as rheumatoid arthritis, lupus (SLE) or vasculitis. These conditions lead to inflammation of the blood vessels, hence affecting bloodflow to the inner ear.
Sudden hearing loss also appears to be more common in those with pre-existing health conditions. These include diabetes, high cholesterol and high blood pressure. Smoking may also increase the risk of sudden hearing loss, presumably related to the chronic oxygen deprivation of the delicate inner ear (the nerve centre).
As an ENT specialist with a special interest in hearing and dizzy disorders, I think the top 4 causes for sudden hearing loss are:
- Infection of the inner ear, probably viral
- Vascular or bloodflow issues, such as a microscopic blood clot blocking off the blood supply of the inner ear
- Tumour of the inner ear (acoustic neuroma)
- Nerve-related or auto-immune disease
Syphilis and HIV may also lead to sudden hearing loss, presumably due to the overall inflammation caused by these conditions. Sudden hearing loss can also occur in people who scuba dive, especially to deep depths underwater. High underwater pressure with problems equalising the Eustachian pressure tube, may lead to barotrauma. The delicate inner ear ruptures, causing a small leak of inner ear fluid (perilymph leak).
WHAT IS THE TREATMENT FOR SUDDEN HEARING LOSS?
Sudden hearing loss is SENSORINEURAL, meaning it has occurred in the inner ear nerve centre. It usually has nothing to do with the eardrum or impacted wax. This is even more true, especially if the hearing loss is severe. Simple screening with tuning fork tests can be done by a doctor, especially out-of-hours. The attending doctor needs to decide whether to prescribe a course of oral steroids to treat the sudden hearing loss.
Weighing the risks vs benefits here of oral steroids, many doctors WOULD start the course of oral steroids. This usually consists of prednisolone at 1 mg/kg daily, maximum 60 mg daily, in normal healthy patients. Diabetics should exercise caution, as it will impair the blood sugar control temporarily. Steroids can cause sleep disturbances if taken at night.
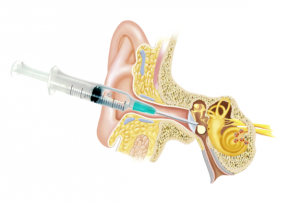
Ultimately, you still need to see your ENT specialist to confirm your sudden hearing loss with a hearing test. Let’s discuss continuing oral steroids or switching to intratympanic steroid injections. The latter aims to deliver the medication through your eardrum (Figure 1). Some patients may choose to have both oral and intratympanic steroids. But others wish to try the oral route first before the eardrum injections are considered.
WHAT ARE INTRATYMPANIC STEROID INJECTIONS?
Intratympanic steroid injections through the eardrum are painless and easily done in clinic. The key is to lie there for at least 30 minutes after the injection. This allows time for the steroid medication to enter the inner ear via the natural inner ear membranes. The number of injections can vary but most ENT specialists in Singapore would probably attempt 3 injections, on a daily or alternate day basis. If there is still no improvement, then there may not be much point having more.
DO I NEED AN MRI SCAN OF MY INNER EAR AND BRAIN?
The most important investigation is an MRI scan of your inner ear. This is done to exclude the presence of an inner ear tumour, called an acoustic neuroma. This is a benign nodule of the balance nerve which is sometimes detected as an incidental finding on MRI scans performed for other reasons. Acoustic neuromas are associated with 15-20 % risk of sudden hearing loss. So this may be your first presentation of an acoustic neuroma which previously did not cause any symptoms as it was still small.
Conversely, we find acoustic neuromas as the cause of about 2% of sudden hearing loss cases. Even if your sudden hearing loss seems to improve, please still have your MRI scan. Steroids can temporarily shrink the neuroma, making the hearing loss recover. But it won’t make the underlying neuroma disappear. If you omit your MRI scan, you cannot rule out the acoustic neuroma. So please have your MRI scan of the inner ears.
WHAT HAPPENS IF THE SUDDEN HEARING LOSS DOES NOT RECOVER?
The peak time for recovery for sudden hearing loss seems to fall around the 2-3 week mark. But delayed recovery can still occur. So what happens in the worst case scenario? You have tried everything, including hyperbaric oxygen therapy, vitamins, antivirals, steroids and aspirin. There are at least 1000 different ways of sudden hearing loss treatment in the literature! Unfortunately, none are proven for sure. But steroids would probably be the one treatment which most ENT specialists would agree on.
If you only have partial hearing loss in one ear, a standard hearing aid may help. If the hearing loss is more severe, then a different hearing aid called a CROS hearing aid may help. This reroutes the sound from your bad side over to your good ear. In my experience, CROS hearing aids are not popular. Why? They don’t seem to provide much benefit for the patient with single sided deafness. Such patients tend to compare the hearing in their bad ear to their good ear and are seldom satisfied. They are also more expensive than standard hearing aids.
When hearing aids don’t work out, then next up is the option of hearing implants. Hearing implants come in the form of a Bone-Anchored hearing implant such as a BAHA or Bonebridge, OR a cochlear implant. Each option has its pros and cons. You would only consider hearing implants if there was no improvement in sudden hearing loss after at least 6 months.
WHAT IS A BONE-ANCHORED HEARING IMPLANT?
A Bone-Anchored hearing implant such as a Bonebridge is easy to insert. A Bonebridge provides immediate hearing benefit once switched on. You won’t need much speech rehab at all. But it doesn’t provide true sound! It reroutes the sound entering the good ear over to the bad ear, via conduction through the skull bone. It helps to provide “surround sound” hearing for both ears, localising sound better. So you should find it easier to hear in a noisy place. Surgery is short and can be done as a day case.
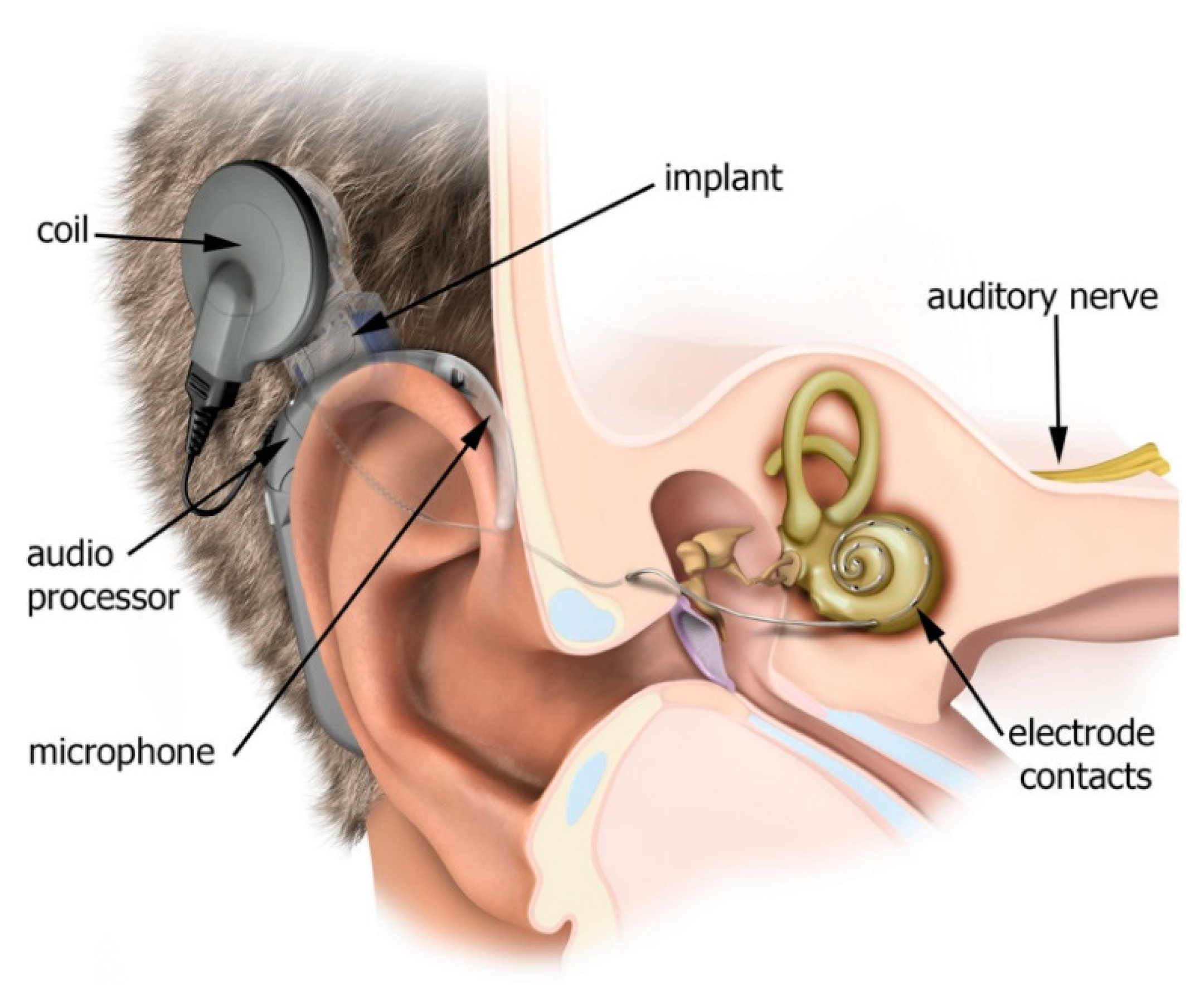
A cochlear implant (below), on the other hand, requires more complex longer surgery. This takes about 2-3 hours and needs speech rehab to retrain the inner ear to process speech. In adults who already have good language skills, the rehab is much faster. It involves inserting a long electrode directly into the inner ear nerve centre, the cochlea. Electrical signals are now sent to the hearing nerve, providing true sound.
So there you go, everything you need to know about sudden hearing loss! Remember, that early treatment is critical for optimal recovery of sudden hearing loss. Please seek medical attention even if it’s out-of-hours, at your emergency department or urgent care centre. At the very least, a course of oral steroids can be started early. Don’t forget to follow up with your friendly ENT specialist in Singapore!
Share this blog via: